
Transitioning to competency-based education in nursing: a scoping review of curriculum review and revision strategies | BMC Nursing

This scoping review included 37 studies published between 2011 and 2024, representing a broad international scope. The geographic distributions include 15 studies originated from the Global North (including the USA, Canada, Australia, and Germany), 11 from the Global South (such as India, Iran, Saudi Arabia, and Thailand), and the remaining studies were global or conceptual reviews not tied to a specific country. The majority employed descriptive and cross-sectional designs, while others used quasi-experimental, pretest-posttest, systematic reviews, concept analyses, and curriculum development approaches. These comprised 12 review papers (systematic, scoping, or narrative), 7 cross-sectional surveys, 4 quasi-experimental or pretest-posttest studies, 3 descriptive studies, 3 concept or literature analyses, and 8 other studies, including pilot programs, practice updates, and curriculum development initiatives. Sample sizes varied significantly, ranging from small groups to large-scale studies involving over 25,000 participants.
The studies addressed key themes such as competency framework development, evidence-based practice integration, simulation and technology in teaching, peer-assisted learning, cultural competence, and curriculum reform. Together, they provide a comprehensive view of how CBE is implemented and evaluated in nursing.
The components of CBE emerged in three aligned domains that included the following: Curriculum Design, Teaching methods, and Assessment. CBE is grounded in predefined competencies derived from real-world job requirements and professional standards. These competencies include a broad spectrum of abilities, encompassing not only clinical skills but also critical thinking, decision-making, ethical practice, and communication [17]. By orienting the educational process around these competencies, programs ensure that theoretical knowledge is seamlessly integrated with clinical practice. The components of CBE emerged in three aligned domains that included the following.
Curriculum design
Curriculum design in competency-based education (CBE) is grounded in the systematic development of measurable, practice-based competencies that align with the realities of clinical practice and healthcare delivery. Unlike traditional education models that emphasize subject content, CBE shifts the focus toward the end capabilities of graduates—what students must know and be able to do upon program completion [17, 18]. These competencies span a broad range of domains, including clinical proficiency, critical thinking, professional ethics, interprofessional collaboration, and cultural competence.
As illustrated in Fig. 2, curriculum design in CBE follows a backward design model [19], where the end goals (competencies) are defined first. The learning experiences, teaching strategies, and assessments are then aligned to ensure students acquire those specific competencies. This approach guarantees that every educational element is purposefully crafted to support the final outcomes expected from graduates [20, 18].
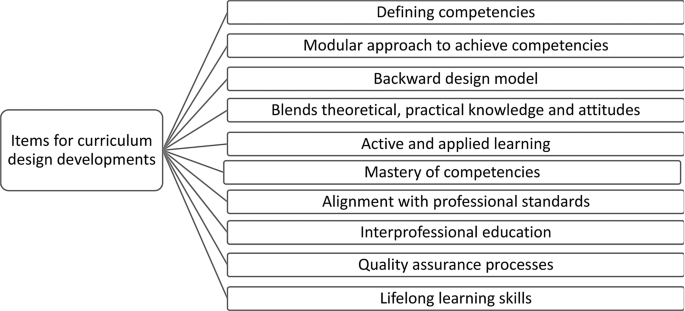
Items for curriculum design developments
The curriculum is often organized into modular units, each representing a specific cluster of competencies. This modular structure not only enables focused instruction and precise assessment but also supports personalized learning—allowing students to progress at their own pace based on demonstrated mastery [21, 22]. It enhances flexibility and responsiveness to individual learning needs.
Incorporating active and applied learning opportunities is a core feature of CBE curriculum design. Simulations, practicums, role-playing, and project-based learning are embedded to ensure students engage directly with real-life clinical contexts [20]. This experiential approach strengthens skill acquisition, decision-making, and situational awareness.
To ensure relevance and rigor, the curriculum must align with professional and accreditation standards, ensuring that graduates meet regulatory and workforce expectations [20]. Additionally, lifelong learning is a built-in principle in CBE curriculum design. It encourages students to adapt continuously, pursue ongoing professional development, and remain current in their competencies across their careers [23, 22].
CBE curricula increasingly emphasize interprofessional education (IPE), allowing learners to collaborate across disciplines. IPE builds communication, respect, and coordination in healthcare teams, ultimately improving patient outcomes [24, 25]. Moreover, quality assurance mechanisms—such as periodic curriculum reviews and stakeholder feedback—help ensure continuous alignment with healthcare innovations and evolving practice environments [26]. See Fig. 2: Key Components of Curriculum Design in CBE
Teaching methods
The success of competency-based education depends not only on what is taught but also how it is taught. CBE employs a wide range of learner-centered and outcomes-focused teaching methods that promote deep learning, critical thinking, and skill mastery. As illustrated in Fig. 3, these methods are selected and structured to ensure alignment with competency outcomes [27].
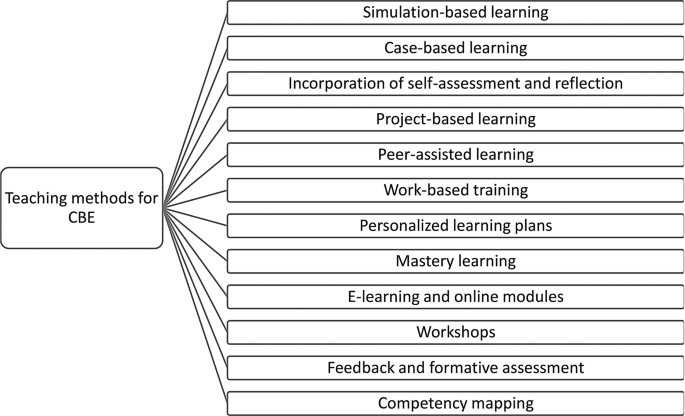
Simulation-based learning is a hallmark strategy in CBE. It immerses students in realistic clinical scenarios using high- or low-fidelity mannequins and digital tools, allowing them to practice skills, make decisions, and learn from mistakes in a risk-free environment. Simulations enhance student competence, confidence, and readiness for clinical settings [28]. Similarly, case-based learning (CBL) enables students to solve patient care problems by applying theoretical knowledge to complex, real-world scenarios. This method promotes critical thinking and clinical reasoning [29].
Project-based learning (PjBL) facilitates the integration of multiple competencies over time. Students engage in extended, often interdisciplinary tasks that simulate professional challenges and require collaboration, problem-solving, and reflective thinking [30]. Peer-assisted learning supports mutual learning through group discussions, peer teaching, and collaborative problem-solving, enhancing interpersonal and teamwork skills [25].
To bridge the gap between theory and practice, work-based learning (e.g., internships and practicums) places students in authentic healthcare environments under professional supervision. These experiences allow students to apply competencies in real-time and receive direct feedback from preceptors [31].
Recognizing the diverse needs of learners, CBE also incorporates personalized learning plans, which adapt learning pathways to students’ prior knowledge, learning styles, and individual goals [32, 33]. Mastery learning ensures students fully understand and demonstrate competencies before progressing to the next stage. This supports learning depth, minimizes gaps, and fosters a strong foundation for clinical practice [34].
Technology-enhanced learning, including e-learning platforms, digital simulations, and mobile apps, extends access and flexibility, allowing learners to engage with content at their own pace [35]. Supplementing these are workshops and skills labs, which offer targeted instruction on specialized clinical techniques and procedures [36].
Effective CBE teaching also relies on formative assessment and feedback mechanisms. Continuous feedback loops support improvement, reinforce learning, and align with the principles of transparency and self-directed development [37, 38]. (See Fig. 3: Teaching Strategies Supporting CBE Implementation)
Assessment
Assessment is a critical component of CBE, as it serves to verify whether learners have achieved the intended competencies in meaningful and measurable ways. Unlike traditional education, which may rely heavily on exams, CBE utilizes performance-based, continuous, and multidimensional assessment strategies [27]. Figure 4 outlines key methods used to evaluate student competence in CBE programs.
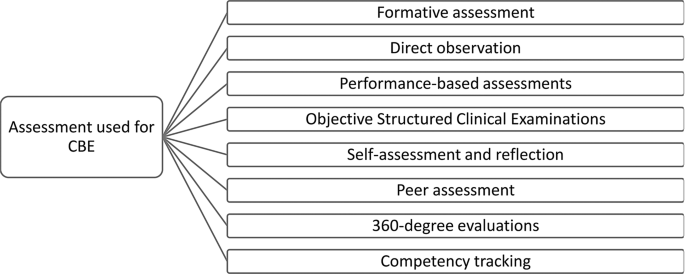
Formative assessments are used throughout the educational journey to monitor progress and provide real-time feedback. These may include quizzes, reflective writing, skill checklists, and verbal feedback during practical tasks. The goal is to guide improvement without contributing heavily to final grades [38]. Summative assessments, on the other hand, are conducted at the end of a learning cycle to determine whether students have mastered required competencies.
Performance-based assessments are central to CBE and include direct observation, clinical simulations, and real-world tasks. These assessments measure how students apply their knowledge and skills in authentic or simulated contexts [39]. One widely used method is the Objective Structured Clinical Examination (OSCE), which requires students to complete a series of timed stations demonstrating different clinical skills. OSCEs offer structured, consistent, and observable measures of student performance.
Other assessment strategies include self-assessment and reflective practice, which encourage learners to critically evaluate their progress and identify areas for growth. This enhances metacognition and promotes lifelong learning [40]. Peer assessments and 360-degree evaluations (involving peers, instructors, and sometimes patients) provide broader perspectives on student performance and encourage accountability and professionalism.
Portfolios serve as longitudinal records of learning and achievement, capturing clinical logs, case reports, skills checklists, and reflective narratives. These artifacts help track development over time and support holistic evaluation [40]. Increasingly, institutions are turning to digital competency-tracking systems that allow for real-time monitoring of learner progress, automated feedback, and integration with curricular goals [21].
To maintain fairness, transparency, and academic integrity, all assessment tools must be valid, reliable, and aligned with the defined competencies. Assessments should not only test what learners know but also how effectively they apply that knowledge in clinical or professional contexts. Well-structured assessments support both learning and accountability, ensuring that graduates are fully prepared to meet the demands of modern healthcare. (See Fig. 4: Assessment Methods in Competency-Based Education)
Advantages of competency-based education
CBE is specifically tailored to align with the needs of the healthcare sector, ensuring that healthcare professionals are competent to provide effective patient care and healthcare delivery (Cate et al., 2016). This educational approach offers several advantages, including preparing graduates more adequately for clinical practice due to demonstrable competence in necessary roles and tasks [27]. CBE also addresses the skill gaps often found between acquired education and real-world requirements, leading to a more capable health workforce (Cate et al., 2016). The efficiency of CBE programs is enhanced as they concentrate on essential competencies, avoiding irrelevant content and stressing core skills and knowledge acquisition. The flexibility of CBE supports personalised learning, allowing students to progress at their preferred pace and catering to unique learning needs. Assessment within CBE is more objective, with clear performance expectations that facilitate transparent assessment [27]. Moreover, CBE encourages lifelong learning, instilling a continuous cycle of competence assessment and improvement throughout professional careers (Cate et al., 2016). (See Fig. 5: The advantages of CBE)

Advantages of Competency-Based Education
Challenges to curriculum revision
Educational institutions pursuing curriculum enhancements in nursing face various resource limitations, where financial constraints and a deficiency of human capital commonly impede the ambit and profundity of potential improvements. [41] have pinpointed these scarcities as significant barriers to advancing educational objectives. Furthermore, an inherent resistance to change within institutions poses a formidable challenge, necessitating faculty development to address the hesitations and to foster an environment that is receptive to transformation, and it illustrates the friction between the demand for progress and an institution’s ability to adapt [42].
The workload associated with curriculum revision is substantial, creating time constraints for faculty members who must balance these efforts with their existing academic and administrative duties [41] Lastly, the integration of technology in nursing curricula presents its own set of challenges. [43] highlight the obstacles of assimilating digital tools, which extend to securing access, establishing appropriate training facilities, and ensuring ongoing support for both faculty and students to utilise new technologies effectively, all of which are essential for contemporary nursing education to progress.
Strategic recommendations
Based on the reviewed literature, the following strategic recommendations can be proposed for effective curriculum revision:
-
Stakeholder Engagement: Engaging stakeholders such as faculty, students, and healthcare industry partners is essential for a responsive curriculum that aligns with real-world needs [44, 45, 46].
-
Curriculum Reform Committees: Forming dedicated committees with broad representation can facilitate focused curriculum revision efforts and ensure diverse perspectives are considered [44, 46].
-
Needs Assessment: Conduct a comprehensive needs assessment to identify gaps, areas for improvement, and emerging trends in nursing education [47]. Conducting a thorough needs assessment, including input from stakeholders, can identify areas for improvement and guide curriculum revision priorities [47].
-
Continuous Evaluation and Feedback: Implementing a system for ongoing evaluation and feedback can ensure that the curriculum remains relevant and effectively addresses the learning objectives [45].
-
Flexible and Modular Curriculum Design: Adopting a flexible and modular curriculum design allows for easier updates and modifications in response to changing healthcare needs and advancements [48, 46].
-
Emphasis on CBE: Shifting the curriculum towards a CBE approach can ensure that graduates possess the necessary knowledge, skills, and attitudes required for nursing practice [49, 27].
-
Faculty Development: Providing faculty with ongoing professional development opportunities, including training on curriculum design and teaching strategies, can enhance their capacity to effectively implement and sustaining them within the broader scope of nursing education [45, 50].
-
Integration of Technology: Incorporate digital tools, simulations, and virtual learning experiences to enhance student engagement and provide practical skills training [51]. A significant number of sudies emphasised the role of digital tools and simulations in enhancing the learning experience and offering students hands-on practice in a controlled environment [52].
-
Alignment with Accreditation Standards: Curriculum revisions must consider current accreditation requirements to maintain the quality and recognition of the nursing program [45]
-
Integrating cultural competence into nursing education is essential to ensure nurses can provide care with a deep understanding of the multitudinous cultural contexts they will work in [33, 24].
link






